Renal Menifesations of Systemic Lupus Erythematous
This is my note for a special case of Systemic Lupus Erythematous + Nephrotic Syndrome. We had a patient, whose renal biopsy showed Focal Segmental Glomerulosclerosis(FSGS), which does not fall into any category of lupus nephritis.
What we learned on textbook: Lupus nephritis
Lupus “nephritis” is due to immune complex deposition in different parts of the glomerulus, leading to different clincal symptoms and outcome.
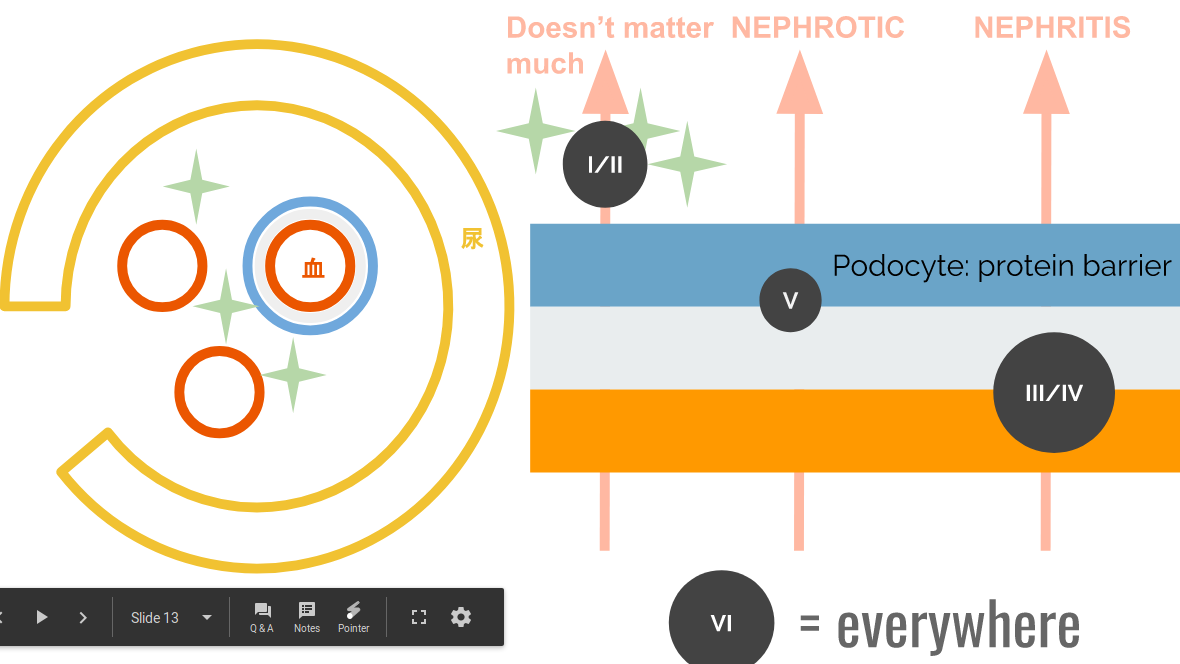
Because podocyte is responsible to filter protein, Destruction of podocyte (type V) usually results in nephrotic syndrome (proteinuria…etc). When demage goes to the capillary, red blood cells pass, and thus, hematuria.
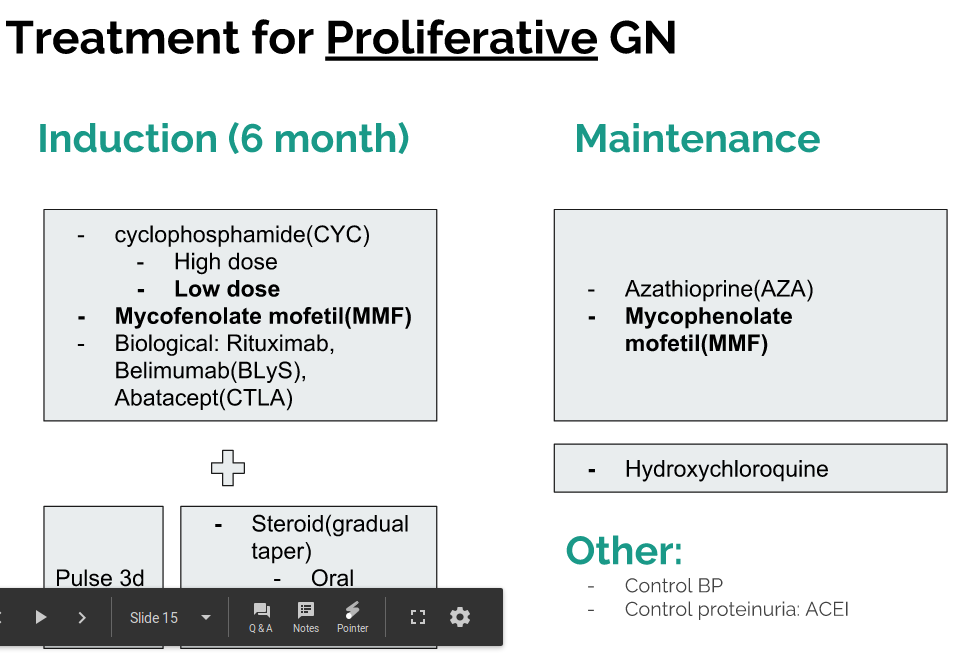
Treatment indication?
And out of the 6 types, type III/IV indicates high dose corticosteroid.
Don’t treat type VI. It’s already irreversible. The side effect by immunosupressants are not worthwhile.
But SLE can have more than lupus nephritis: podocytopathy
We had a patient, whose renal biopsy showed Focal Segmental Glomerulosclerosis(FSGS). Through a series of literature search, I found, there are other possibilities other than lupus nephritis: the concept of lupus podocytopathy! Check out this review
Unlike lupus nephritis, no immune complex will be found under renal biopsy.
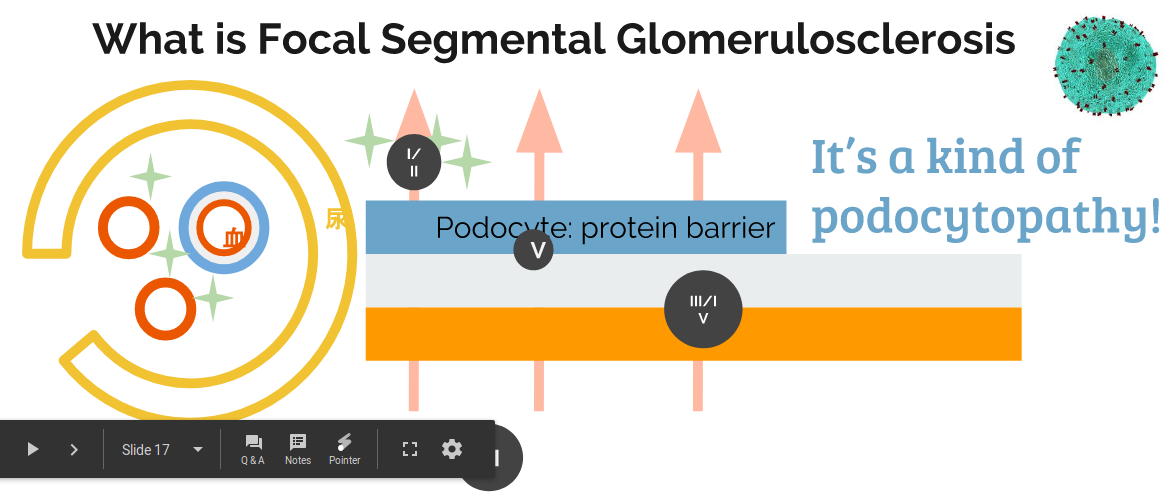 Why did the podocyte got injured? It’s proposed to be related to T cell or soluble urokinase plasminogen activator receptor (suPAR). The pathogenesis in unestablished.
Why did the podocyte got injured? It’s proposed to be related to T cell or soluble urokinase plasminogen activator receptor (suPAR). The pathogenesis in unestablished.
Lupus podocytopathy: Three types
- Minimal Change Disease(MCD)
- Mesangial Proliferative Glomerulonephritis (MsP)
- FSGS
Each has different response to treatment. FSGS is the worst out of three.
Treatment for lupus podocytopathy
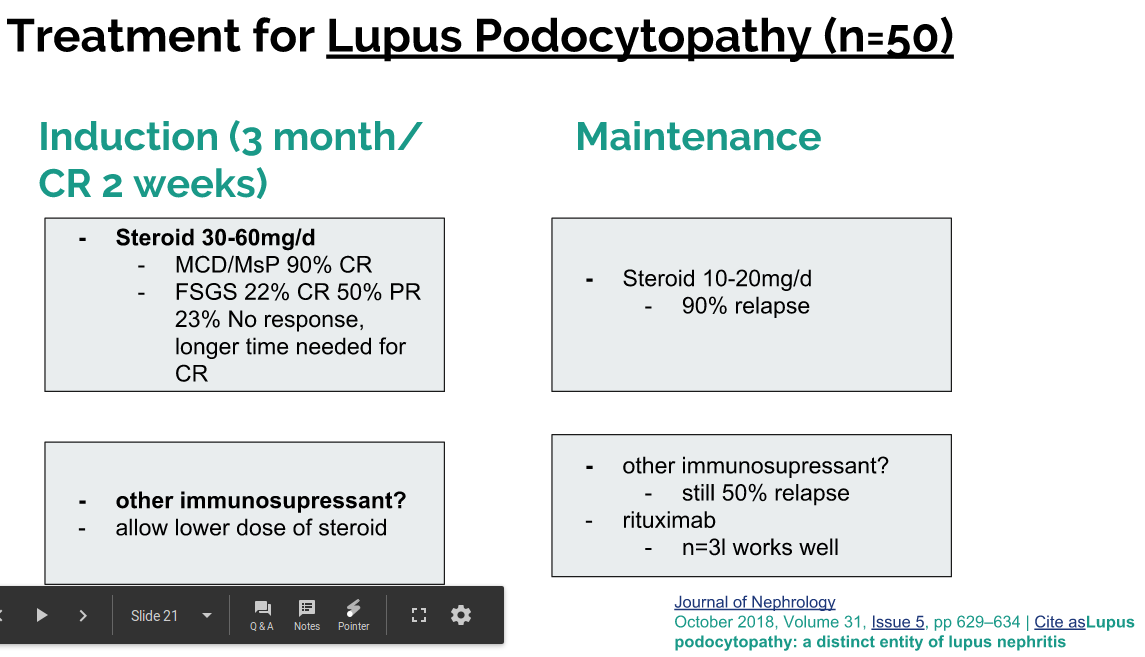
For the maintainence therapy, sole glucocorticoid results in low complete remission and longer time for remission in FSGS. That is why the addition of other immunosupressants are recommended. For induction, sole glucocorticoid is associated with high relapse rate, although additional immunosupressant does not improve outcome. But in the prelimary study, three patient tried rituximab and it turned out better.
Treatment of our patient
- steroid (pulse for 3d + 5mg/d) + cyclosporin 50mg/d
Other Renal Involvement of SLE
- tubulointerstitial
- renal vein thrombosis
- thrombotic microangiopathy: HUS; TTP
Conclusion
- lupus nephropathy = nephritis + podocytopathy + other…
- Treatment depends on biopsy.